Abstract — American bioethicists have been providing persuasive arguments for rationing medical care via the theory of the necessary “rational allocation of nite health care resources.” Anticipating the need for the drastic rationing of medical care in the U.S. with the implementation of ObamaCare and assisted by various sectors of organized medicine in league with the State, bioethicists have deduced that more ingenious approaches are necessary to convince Americans who have been accustomed to receiving the best medical care that third‐party payers are willing to pay for. It is in this context that the individual‐based, patient‐oriented ethics of Hippocrates, including his fundamental dictum, “First Do No Harm,” have to be supplanted by the utilitarian approach promoted by the bioethicists. And today’s foremost proponent of the bioethics movement is Dr. Ezekiel Emanuel. This editorial proposes a rational rebuttal to Dr. Emanuel’s proposal to limit life expectancy to age 75 as a rational paradigm to a better life.
For several decades, American bioethicists have been providing persuasive arguments for rationing medical care via the theory of the necessity of the “rational allocation of finite health care resources.”(2) More recently, assisted by various sectors of organized medicine, they have developed multiple approaches to justify what they see as the necessary curtailment of services and specialized treatments deemed not medically necessary. The problem persists, though, and the need for rationing health services in increasingly socialized medical systems, including ObamaCare, requires more ingenious approaches, particularly in the U.S., where patients are accustomed to receiving the best medical care that third-party payers are willing to pay for, regardless of whether the payer is the insurance company or the government.(6)
Furthermore, government planners, supported by the ever-accommodating bioethicists, posit that with increasing longevity and augmentation of the population of American elderly, more drastic actions will be required to prevent the bankruptcy of the public financing of medical care. They believe therefore that outright government-imposed euthanasia, not only for the terminally ill but also for the inconvenient infirm and the superfluous elderly, will become necessary.(1,4,8,10)
It is in this context that the individual-based, patient-oriented ethics of Hippocrates, including his fundamental dictum, “First Do No Harm,” are seen as an obstacle by the bioethics movement. Obtrusive and in their way, time-honored medical ethics are being eroded and supplanted by the more convenient, collectivist, population-based ethics propounded by today’s bioethicists.
As early as the 1980s, some bioethicists, including Daniel Callahan, then Director of the Hastings Center; Peter Singer, bioethics professor at Stanford University; and John Hardwig, Professor of Ethics at the University of Tennessee, openly insisted that elderly patients who had lived a full life had a “duty to die” for the good of society and the proper utilization of societal health resources.(2) Dr. Callahan pointedly asserted, “Denial of nutrition, may, in the long run, become the only effective way to make certain that a large number of biologically tenacious patients actually die.”(11)
Likewise, Dr. Hardwig dropped all pretenses regarding their real intentions at about the time of the Clinton health care debate and the tentative formulation of HillaryCare, affirming a “duty to die” was necessary for those citizens whose lives had become not worth living because of chronic disease or advanced age.(7,10) Such openness was not well-received by the American people, and Hardwig’s proposals were ignored, or like HillaryCare ostensibly discarded, thrown by the wayside. But appearances can be deceiving. Many proposals of the bioethics movement have quietly and gradually been implemented. Here is an insightful report by Pope Benedict XVI in his address to the Pontifical Academy for Life:
“Some ethicists warn that modern bioethics is in fact a new normative system of ethics that, based on principles of utilitarianism, can never be compatible with Natural Law principles. In the last few decades, bioethics has largely supplanted traditional, Natural Law-based medical ethics in hospitals and ethics boards in most western countries. Under traditional medical ethics, the guiding principle is ‘do no harm.’ But contemporary bioethics abandons this…in an effort to find the utilitarian goal of the ‘greatest good for the greatest number.’ Under these principles, preserving the life of the human patient is not considered paramount.”(12)
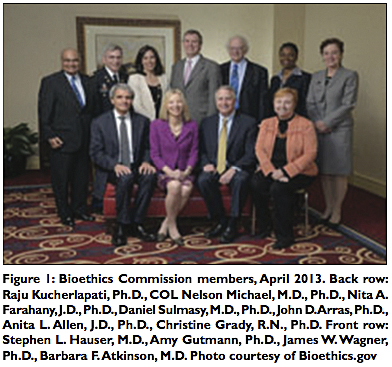
Benedict XVI is largely correct in his assessment. Moreover, the bioethics movement has recently received more impetus with President Barack Obama’s creation of the Presidential Commission for the Study of Bioethical Issues [Figure 1].(9)
But their proposals have not all been fully implemented. To do so, today’s bioethicists, although equally determined, are more subtle, and the foremost exponent of the new trend in bioethics is Dr. Ezekiel J. Emanuel.(3) Although 57 years of age and in good health, Dr. Emanuel says he hopes and wants to live to age 75 and die. He has lived a fulfilled and a good life and it is time to exit. After age 75, Emanuel claims life is a downhill spiral and not worth living. His family disagrees with him and says he is “crazy,”(3) yet the fact remains Dr. Emanuel is a respected bioethicist, the Director of the Clinical Bioethics Department at the U.S. National Institutes of Health, the recipient of numerous awards, but the danger here is he encapsulates the views many bioethicists hold today. He insists that the productivity of creative people [Figure 2] reach a peak at age 40 and plateau by age 60. In other words, after age 60, even productive people, create and produce little of value to society.(3) I beg to differ. In a recent conversation with my friend Dr. Russell Blaylock, who has also written on this subject,(1) he opined, “The reason very smart, creative people no longer produce earth-shattering discoveries later in life is because after their great accomplishments, they become department heads, drowning in administrative duties that prevent creative activities.” I agree with Dr. Blaylock. Moreover, as we age and mellow and reach retirement, we also achieve satisfaction from a productive life well spent, and begin the contemplation and enjoyment of life that is only possible with the leisure that comes with retirement.
Dr. Emanuel, in stressing the relatively young age in which productive people reach the apex of their creativity, e.g., novelists, poets, and physicists, argues as if becoming poet laureates and Noble Prize winners were the universal aspirations of the average citizen. Most people do not aspire to reach those dizzying heights! The more realistic goals in life, instead, are more mundane, namely, fulfillment and contentment, qualities that are attained by being good citizens, and the satisfaction of leading good and productive lives; men and women performing their occupations and respective jobs, whether menial, artistic or intellectual, and doing them well — in short, being the best we can be in this transitory phase of our existence!
In his article Dr. Emanuel writes that if we live longer than age 75, “we are no longer remembered as vibrant and engaged but as feeble, ineffectual, even pathetic.”(3) And as far as suicide or euthanasia, Dr. Emmanuel claims he is against those options, although it escapes him logical reasoning will lead many people to pursue exactly those options when afflicted with depression, physical illness, or merely reaching that lethal age of 75 — or even worse. By which I refer to the State compulsorily implementing exactly those policies, purportedly as pragmatic and “sound” health care policies, when in fact they may be implemented for political expediency or budgetary considerations. This is particularly ominous when the State is involved in administering and funding medical care, as in socialized medicine or ObamaCare.(6,7)
In the same vein toward the end of his paper, Dr. Emanuel claims he is not advocating compulsory end of life at age 75 “in order to save resources, ration health care, or address public-policy issues,” but that is exactly what he is inferring. In fact, in the next breath, he admits his proposals do have at least two policy implications and that these implications do refer to reducing life expectancy.(3)
Dr. Emanuel complains that Americans are obsessed with performing physical and mental exercises, undertaking diets, taking vitamins and supplements, “all in a valiant effort to cheat death and prolong life as long as possible.”(3) In fact, leading healthy lifestyles and sticking to healthy diets are exactly what Americans should be doing, not only to prolong their lives, but even more importantly to improve the quality of their lives, while saving their own health care costs.
“Doing mental puzzles,” which people have done to exercise brain function [Figure 3] and which Dr. Emanuel derides,(3) may not exactly translate to the highest intellectual exercise. But not so other intellectual pursuits. I refer to reading and studying the classics of history and literature for their own sake; listening to good music in moments of contemplation for mere enjoyment; spending more leisure time with our families — in short enjoying all of those happy activities of leisure and exercising those fundamental virtues, which eluded us in our earlier, more active and hectic years of youth and adulthood. It is in our advancing years that we have the leisure to spend the time in just those intellectual activities that engage the mind and sooth the soul.
Others find happiness and satisfaction in doing what they have always done in life. This is particularly true of those who have answered a professional calling, who obtain intellectual rewards in continuing to practice their professions to the very end or until they are impaired by age or disability. That was the case with my father, a physician. It is the case, I suspect, with Dr. James I. Ausman, editor-in-chief of Surgical Neurology International, who at age 76 remains a scholar and an incorrigible multitasker and who seems to gather ever more speed in life as he gets older!
The key to meaningful longevity, then, is to remain active, exercising our intellectual faculties for their own sake, as well as for the preservation of brain plasticity. Dr. Emanuel admits the neural connections that are most utilized are reinforced and preserved, while those connections and synapses not used degenerate and atrophy. However, he is incorrect when he states that we cannot learn as we get older because no new neural connections and re-wirings are possible. Brain plasticity allows us to continue to learn well beyond age 75 [Figure 4] for those who remain active, although it is true that in extremely advanced age, learning, creative thoughts, and memory retention become progressively more difficult as degeneration of neural connections and neuronal death take place.
Thus, I am curious as well as perplexed. Has Dr. Emanuel ever had the interest or time to read Thucydides and Herodotus? I wonder if he ever read Plutarch, Livy, Virgil, or any of the poems of Sappho or Elizabeth Barrett Browning? I wonder if he ever read Plato, Aristotle, or understands the meaning of the Aristotelian good life [Figure 5], and the time and activities that are necessary for the attainment of real happiness and wisdom? The ultimate good life is not necessarily found in our hard-working, intensive, utilitarian, and productive years, but in our years of leisure and contemplation that in today’s stressful and fast-moving society can be attained only in our advancing years. One can also spend those years continuing to fulfill the duties of citizenship, improving his/her communities, insisting on better government — e.g., preserving and increasing liberty — for one’s children and grandchildren, hoping they live in a better world. In this sense, Dr. Emanuel’s attitude reflects selfishness and lack of concern for the welfare of others around him or who may come after he’s gone! Contrary to Dr. Emanuel’s opinion about “faltering and declining” years past age 75, it is idleness, selfishness, and wasteful lives associated with diseases of the soul primarily that are the culprits for moral and intellectual decrepitude, rather than physical decline and reaching a certain capricious chronological age.
I’m not arguing here against individuals exercising their right to medical autonomy, especially those suffering from chronic disease and terminal illness. End-of-life decisions should be left to individual patients, their families, and their physicians. What I’m saying is that lives can be productive and fulfilling, worthy of living past age 75. I’m also cautioning bioethicists from propounding the utilitarian concept of “a duty to die” because a certain lethal age has been reached or chronic illness has become manifest. We cannot separate, nor does Dr. Emanuel distinguish, the process of aging from infirmity and illness. Certainly one leads to the other, and the duty to die at age 75 becomes the duty to die at any age, once a life is deemed not worth living. Death then is prescribed by the government planners and the doctors and bioethicists employed by the State, whether one reaches a certain age or is afflicted by illness.(1,4,8-11)
With the advances in medical care, life expectancy has been prolonged and the quality of life has been made immensely better. Yet, Dr. Emanuel argues: “Since 1960, however, increases in longevity have been achieved mainly by extending the lives of people over 60. Rather than saving more young people, we are stretching out old age.” Furthermore, he asserts this is wrong because we are saving the life of older people with a myriad of medical problems and residual disabilities.(3) While, I admit this is partly true, many of these people can be returned to normal or near normal life with proper medical and nursing care. Moreover, medical and Judeo-Christian ethics, not to mention the lessons of history, have taught us that we should treat with compassion the sick and the most vulnerable segments of our society. Societies that do not do this descend into cruelty and barbarism. Once again, we must recollect the lessons of fairly recent history. Dr. Leo Alexander, the leading psychiatrist and Chief U.S. Medical Consultant at the Nuremberg War Crimes Trials [Figure 6], in his classic 1949 New England Journal of Medicine article described how German physicians became willing accomplices with the Nazis in Ktenology, “the science of killing.” This was done, we learn, for the good of German society and the improvement of “the health of the German nation.” And in this light, Dr. Alexander asked the critical question: “If only those whose treatment is worthwhile in terms of prognosis are to be treated, what about the other ones? The doubtful patients are the ones whose recovery appears unlikely, but frequently if treated energetically, they surprise the best prognosticators.” Once the rational allocation of scarce and finite resources enters the decision-making process in the doctor’s role as physician, the next logical step is: “Is it worthwhile to do this or that for this type of patient,” or for those who have reached a certain age?(5)
As much as Dr. Emanuel insists he is against euthanasia, his arguments lead inexorably to utilitarian ethics, the idea of lives deemed not worth living, and ultimately to euthanasia. Under the utilitarian ethics of the rational allocation of resources, productive lives whose only merit was considered benefit to society, Hitler issued his first order for active euthanasia in Germany on September 1, 1939. And yet it must be pointed out the road to euthanasia was paved before the Nazis came to power. German physicians in the social democracy of the Weimar Republic, as early as 1931, had openly held discussions about the sterilization of undesirables and euthanasia of the chronically mentally ill. So when the National Socialists (Nazis) came to power, “humanitarian” groups had already been set up, ostensibly for the promotion of health. These misguided groups with arguably “good intentions” had taken the first steps and were very useful serving as cover for the subsequent Nazi mass-killing program. And so it was that years before the onset of World War II and the Final Solution had been implemented, 275,000 non-Jewish citizens were put to death in Germany’s “mercy-killing” program. From small beginnings and seemingly “well-intended” proposals, the values of the medical profession as well as an entire society were (and may be again) subverted by deliberately evil or misguided, well-intentioned men working in tandem with the State. Dr. Alexander was correct: “Corrosion begins in microscopic proportions.”(5)
In conclusion, the resurgent bioethics movement — stressing “futility of care,” conservation of resources, and “the duty to die,” while rejecting Hippocrates’ dictum of “First Do No Harm” and refusing to stand for what is in the best interest of the individual and the dignity of human life — is transmogrifying the time-honored, individual-based, patient-oriented medical ethics of Hippocrates into a collectivist, population-based ethic derived from the current thinking of the bioethics movement in the United Kingdom and most of Europe, as well as the United States. This resurgent ethic, presently propounded with subtle and dissimulating persuasion, is particularly well exemplified by Dr. Ezekiel Emanuel, today its foremost proponent. This bioethics “duty to die” movement is buttressed by a utilitarian, population-based ethic concerned primarily with the conservation of resources in the administration of socialized medicine by the State, rather than with the individual patient — and represents the first step down the slippery slope of determining who lives and who dies, rationing by death, and euthanasia. Doctors, patients, and the public at large must be made aware of the direction present society is headed.
Read the follow up to this article on compression of morbidity and longevity
References
1. Blaylock RL. HaciendaPublishing.com, September 26, 2009.
2. Callahan D. Setting Limits, Medical Goals in an Aging Society. New York: Simon and Schuster, 1988.
3. Emanuel EJ. : An argument that society and families — and you — will be better off if nature takes its course swiftly and promptly. The Atlantic, September 17, 2014.
4. Faria MA. . HaciendaPublishing.com, October 24, 2012.
5. Faria MA. . Medical Sentinel 1998;3(3):79-83
6. Faria MA. . GOPUSA.com, March 18, 2010.
7. Faria MA. . Surg Neurol Int 2012;3:71.
8. Faria MA. . Medical Sentinel 1999;4(6):208-210.
9. Faria MA. The road being paved to neuroethics: A path leading to bioethics or to neuroscience medical ethics? Surg Neurol Int 2014;5:146. Available from: [Last accessed on 2014 Oct 7].
10. Smith WJ. : The Assault on Medical Ethics in America. San Francisco, CA, Encounter Books, 2000.
11. Wickham ED. — The Third Path to Imposed Death. Presented at the Annual Life Conference Raleigh, North Carolina, October 23, 2010. Citing Bioethicist Daniel Callahan, 1983, “On Feeding the Dying,” Hastings Center Report 13(5):22.
12. Wickham ED. — The Third Path to Imposed Death. Presented at the Annual Life Conference Raleigh, North Carolina, October 23, 2010. Citing Pope Benedict XVI’s 2010 address to the Pontifical Academy for Life.
Written by Dr. Miguel A. Faria
Miguel A. Faria Jr., M.D. is Associate Editor in Chief and World Affairs Editor of Surgical Neurology International. He is a former Clinical Professor of Neurosurgery and Adjunct Professor of Medical History. Dr. Faria is the author of Cuba in Revolution — Escape From a Lost Paradise (2002). He has written numerous articles on the blessings of liberty and the venalities of totalitarianism, collectivism, and communism — all posted at his website: https://haciendapublishing.com/
This article can be cited as: Faria MA. Bioethics and why I hope to live beyond age 75 attaining wisdom! — A rebuttal to Dr. Ezekiel Emanuel’s 75 Age limit. HaciendaPublishing.com, November 5, 2014. Available from: http://surgicalneurologyint.com/surgicalint_articles/bioethics-and-why-i-hope-to-live-beyond-age-75-attaining-wisdom-a-rebuttal-to-dr-ezekiel-emanuels-75-age-limit/
Copyright ©2014-2016 Miguel A. Faria, Jr., M.D.