
In Part 2, we debunked propaganda, erroneous claims, and phony statistics cited by obfuscating, socialized medicine proponents to tar the U.S. health care system. In Part 3, we continue to debunk misinformation and describe how government interference in the medical marketplace has contributed to, and in certain instances even created, the problems we are experiencing today. Yet, Democrats and proponents of socialized medicine insist more government is needed, and that ultimately the single payer system is the solution. Factoids, misinformation, phony claims and misleading statistics are all used in that effort.

When it comes to health statistics, one must ascertain that the data cited have not been . The U.S. public health establishment has become a willing vehicle because it has become so politicized that figures and statistics must be checked and double-checked, especially when it concerns social and economic issues impacting on health care policy. And make no mistake about it, more than ideology plays a role; the , so intertwined with financial self-interest, is also a major consideration for these “public servant” health officials.
Returning to their criticism of the U.S. health care system, an article by an American economics professor characteristically remonstrated, “administrative complexity and waste are no accident but rather are baked into our private health insurance system and made worse by continuing attempts to use competitive market processes to achieve social ends other than maximizing profit.”
But U.S. private health insurance “are baked” in complexity and bureaucracy, not because market forces are at work but precisely the opposite: Health care is probably the most extensively government-regulated industry in the U.S. The solution offered by this professor is, predictably, the adoption of the government as the single payer! Why would the government do a better job with the health care industry than it has done with every other business, industry, or profession, other than defense, in which it has inserted itself with disastrous consequences? We are left to wonder.
Another article by CBS News states: “Medical care prices increased 4 percent in 2016 according to the Bureau of Labor Statistics, and premiums under Obamacare’s second-lowest costing “silver” plans rose 7.5 percent in 2015. Plus, the U.S. spends far more per capita on health care — $9,892 in 2016 — than any other nation.” All this is true, and the article correctly cites some of the reasons why medical care is expensive. Unfortunately, the first factor listed, “high administrative costs” fails to identify the real culprit; instead, like the previous writer, the CBS article blames high administrative costs on the “U.S. having so many payers — from a slew of private health insurance companies to government programs — that physicians have to negotiate with in the regular course of business.”
High administrative costs are the result of government imposed regulations, such as waiting on the phone for authorization for medical testing and procedures, approval for hospitalizations, hospital days, etc., and for this rigmarole an excessive number of billing clerks and bureaucracy is needed. These regulations begin with Medicare and Medicaid to reduce costs, paradoxically, and soon enough find themselves in the business of “private insurance.” Thus, bureaucracy and complexity in the third party payer system is directly or indirectly government related. A “slew of private health insurance companies” is good for the public; it does not increase complexity per se as claimed, because free market competition and variety of choice in insurance plans, if unfettered by government, would increase freedom of choice and reduce costs, as they do in every other industry.
Other pernicious causes of high cost of medical care are the practice of defensive medicine and the high price of technology. The first has been an insoluble problem because the U.S. has more preying lawyers than any other “industrialized nation,” and in litigious America, fishing expeditions and ambulance chasing have sadly become repulsively too common. Trial lawyer advertising in the quest of fomenting an adversarial society, instead of a harmonious one, is another fact of life. Defensive medicine to protect from medical lawsuits, consequently, will persist, until vigorous tort reform is implemented. High technology will result in high costs because we are at the cutting edge of advances, and research and development is expensive.
The article, as mentioned, identifies the problems, but then as if on cue — like some of the other phony claims and leftist rhetoric that we have encountered — calls for socialized medicine. The sophistry used in this fallacious claim is that universal coverage will bring about a reduction in health care costs, asserting, “When countries cover everybody, they then turn to saving money.”
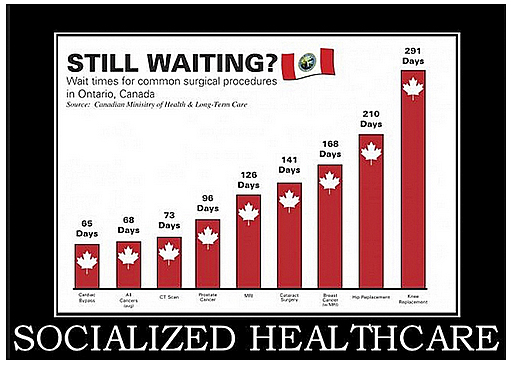
The article, though, leaves out the real and only possible explanation for how nations with socialized medicine save money. They do so by rationing of medical care, as I stated previously: By queues and waiting lists, restrictions to see specialists, limiting access to life-saving medical treatments, cutting back approved services, and even outright denial of services to the most vulnerable in society, those deemed to have incurable illnesses too expensive for the government to allocate resources, and the elderly, after they reach a certain age.
Only as if in passing, the article makes the subtle but astounding admission that some officials recognize the real problem of high medical care costs and are trying to break through the bureaucratic haze to provide real free market solutions: “A few providers in the U.S. and abroad are experimenting with a more direct approach to patients paying for primary care, in which patients pay a monthly fee to the office as they would pay a premium, then pay directly for visits and procedures.” But there the suggestion stops and no effort is made to pursue the thought to its logical conclusion and allow the invisible hand of the free market to function unhindered.
Government is the problem! Reforms are needed but in a completely different direction. We have been traveling in the wrong direction for the last several decades — that is, more and more government intervention, which has worsened the situation that liberals created in the first place and now decry. We need instead more free market incentives and deregulation, and the removal of the monopolistic protection that the government has extended to the big insurance carriers. With these reforms, the health insurance industry would be subject to , improving access and facilitating coverage by making insurance more affordable.
Lack of competition is the major reason, for example, that Health Savings Accounts (HSAs) have not been expanded in many states, remain a very limited option, and truly affordable catastrophic health insurance has not been made available. So, admittedly, there are problems in the health care system, which need addressing. Both medical care delivery and prescription drugs are also too expensive. If costs and bureaucratic red tape could be reduced, the number of the uninsured would further decrease without the need for government compulsion and penalties. Likewise, pharmaceutical competition would bring down the price of prescription drugs. So it’s worth repeating, the underlying cause of dissatisfaction is not that we need more government involvement, but that we need more competition and more free market incentives.
Since third party payers — whether private insurance or government programs — foot most medical bills, doctors and patients do not even discuss fees for elective medical and surgical procedures. The perception (and reality) is that someone else pays the bill, so that both patient and doctor are reluctant to discuss fees, even though 96% of medical encounters are routine, not requiring emergency care.
Just recently in fact, my wife and I had the opportunity to see just how much the invisible hand of the free market has been shackled in the delivery of private, fee-for-service medical care. Asking my wife’s surgeon for his fee for an elective procedure that she was contemplating, he dismissed the question, saying he “didn’t know” and “we needed to ask someone in the business office!” Later, he admitted to us that some dentists and cosmetic plastic surgeons had a competitive and better system because patients pay for their own health care in those settings.
The point in this story is that to bring prices down in our medical care system, as in every other consumer transaction, fees and prices must be discussed to encourage competition.
Here is another story: Another friend, who as an uninsured but prudent consumer of health care (“fee for service” medicine), routinely shops around for the best doctors at the best prices. She needed bunion removal surgery and had it done, after she found the right doctor at the best price. He turned out to be one of the best specialists in town, yet she managed to get a 50% hospital reduction and a 40% doctor’s fee reduction for her surgery and follow-up, post-op care. My wife and I have also experienced major reductions in fees by both doctors and hospitals in other specialties for both diagnostic and therapeutic procedures. In fact, we found other physicians, who were equally price-conscious and happy to help patients obtain competitively priced and equally effective medications, even from other countries for both family and friends. The free market incentive of competition, though, has to be there, promoted by both patients and health care providers, for reducing costs.
It seems insurance companies are disliked by everyone, but unnoticed has gone the fact that hospital costs and doctors fees have increased astronomically. Insurance companies pay this enormous bills and pass the cost to the consumers, accounting for the excessive U.S. health care costs decried by everyone and that compare unfavorably with other countries. This is definitely a problem needing serious addressing, and I venture to say that if politicians do not begin to deregulate the medical industry, and hospitals and health care providers do not help the situation on their own by instituting competition and free market incentives — we could very well end up with the government-run, single payer system. Such socialized national health care system would implement severe rationing, “as in other industrialized countries,” which is the main way they lower costs.
Let me give you now a very critical example. A family friend, who is fully insured, underwent arthroscopic shoulder surgery for a torn rotator cuff ligament. Her surgery lasted 2 hours and she spent another 2 hours at the free-standing orthopedic facility where the surgery was performed. Everything went well and she was pleased with her surgeon. Fees were not discussed. Now hold on to your seat! Her surgeon’s fee was $5,500; the physician assistant, $4,000; the anesthesia was $3,900; the surgical/recovery facility fee was $38,000; the physical therapy and miscellaneous accounted for the rest. Her total bill was $56,000, and there was no hospital stay. Incredible!
How about yet another telling example? The chain free-standing eyeglass facilities have also been getting into the act. I went for a pair of glasses with a supposed promotion I had received in the mail; nevertheless, the price was $500 for a pair of glasses, which I turned down. The optician said, “You have insurance, don’t’ you? I said, “No.” He shrugged and walked away. The optician at my ophthalmologist’s office filled the prescription for $150!
So there you have a more complete picture of what is wrong with the American health care system. It isn’t quality, for we have the best. It is cost, too expensive because of the distortion of the free market largely created by government interference. The solution is to promote free market incentives and encourage competition.
And yet the progressive theoreticians want to overhaul the entire system and throw the baby out with the bath water. In the face of this avalanche of misinformation and misguided solutions — with the free market solutions I’ve outlined elsewhere.
Let’s conclude by remarking on two other comments published in the Telegraph. One of them, who must have been confused, identified the problem with the U.S. health care system as not having enough free market incentives (which is true) as well as being a “medical monopoly” (which is not true) — and then proposed the contradictory and completely wrong remedy: the government as the single payer.
Lastly, there appeared an unsigned editorial on July 29 on The Telegraph (Macon), a McClatchy newspaper. It started correctly stating there had been a lot of debate and then went on to ask, “The essential question is who is going to pay for health care?” A good discussion with factual information followed, but alas, in the end it too sank into partisan emotionalism and class warfare rhetoric: “That brings up other important questions…. What kind of country do we want to be? Do we want to be the kind of country that has a two-tiered health-care system — one for the haves and one for the have-nots that rations care depending on one’s ability to pay?”
We can ask and answer the editorial writer’s repeated question, which he never deigns to answer: “Who pays the bill?” Of course, it would be the overburdened taxpayers, the 53% of citizens who carry most of the federal tax burden.
In response to the rest of his assertion about the two-tiered health-care system, let’s also remind the editorial writer that completely egalitarian systems and free lunches have never existed. In Cuba, there are still two tiers in medical care; one acceptable for the Cuban nomemklatura and the foreign tourists, and another direful one for the people. In Britain, there is the National Health Service (NHS) for the people, and a higher tier and private one for those who can afford it. In Canada, there is the National Health Insurance (NHI) for the proud Canadians, and the American medical care for those who care come across the border. And in China, the “communist” giant, where everyone is supposedly equal, there is a first class and free health care system for the cadres and the princelings, and another direful system that still requires payment for the common people.
And yes, in the freedom of the U.S. health care system, it is better that ability to pay, freedom of choice, and affordability play some role in medical care, as they do with everything else in life— such as food, clothing, housing, funeral arrangements, etc., than having the government, as the single payer, ministering, rationing by death, and deciding who lives and who dies. Just ask the parents of Charlie Gard!
Written by Dr. Miguel Faria
Miguel A. Faria, M.D. is a retired clinical professor of neurosurgery and long time medical editor. He is the author of Vandals at the Gates of Medicine (1995); Medical Warrior: Fighting Corporate Socialized Medicine (1997); and Cuba in Revolution — Escape From a Lost Paradise (2002). His website is
This article may be cited as: Faria MA. U.S. health care debate — Part 3: We need more free market incentives. HaciendaPublishing.com, July 14, 2017. Available from: https://haciendapublishing.com/u-s-health-care-debate-part-3-we-need-more-free-market-incentives-by-miguel-a-faria-md/
Different edited versions of this article with different illustrations have appeared in GOPUSA.com and AIM. The version in AIM was titled, “Tortured Data making health Care Reform Much Harder and appeared on July 24, 2017. The longer version that appears here has been updated and is the same longer version as in The Telegraph (Macon, Georgia) published on August 2, 2017.
Copyright ©2017 Miguel A. Faria, Jr., M.D.