
The act of self-defense can have a double effect: the preservation of one’s life;
and the killing of the aggressor…The one is intended, the other is not.
— Saint Thomas Aquinas
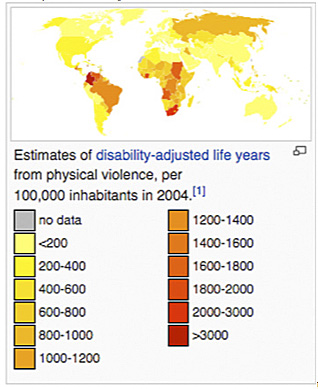
Violence is a global problem, which in the context of this article (interpersonal violence), is intentional force against another person or persons with the potential to cause injury or bodily harm, resulting in disability or death. Despite what one has been led to believe, America is not the most violent nation. [Figure 1] When it comes to violence, objectively compared to developed nations, the U.S. is in the middle of the pack; when considering the rest of the world, the U.S is far behind Latin America (including Brazil), Africa, and much of Eastern Europe and Eurasia (including Russia).
Nevertheless, we must admit that we have an endemic problem that needs addressing. Violence perpetrated by assailants carrying (or having the opportunity to rapidly be able to pick up and use) a blunt object to attack another person may result in severe bodily harm and/or head injury. In the body, severe blunt trauma may result in long bone fractures and external or internal injuries and bleeding—complications requiring surgery by a trauma surgeon. As a neurosurgeon, I’m most familiar with spinal and head injuries, and will reserve these comments to consequences of assaults resulting in severe physical head trauma.
Penetrating head injuries occur with sharp objects forced into the head, such as knives and screwdrivers, both types of tools I have had to remove surgically and in the emergency room under urgent, life-saving circumstances. Most common, though, are blunt traumas to the head of the victim. Penetrating knife injuries and gunshot wounds to the head we will leave for another day.
A stick, bludgeon, or some other solid object can be used against another person. If the head is the target, as it frequently is because of its vulnerability to incapacitation following concussion and loss of consciousness, serious or lethal trauma to the head may result. Blunt head trauma may result in specific injuries, and can with other related injuries of the skull and brain—for example a linear or depressed skull fracture—be associated with a traumatic intracerebral hematoma (brain blood clot), a brain contusion (brain bruise), or a life-threatening epidural hematoma.
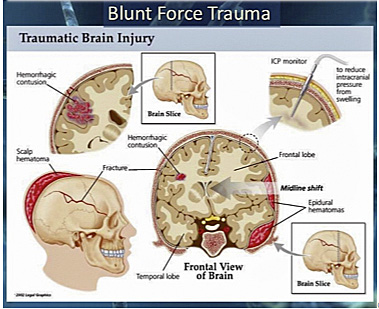
Most depressed (and all open depressed) skull fractures require immediate intervention by the neurosurgeon. The trauma may also cause primary brain damage in the form of a cerebral contusion, or laceration (tearing of the brain), or an expanding hematoma compressing the brain and causing further secondary injury. [Figure 2]
Serious blunt trauma to the head during assaults may result in an expanding hematoma requiring emergency surgery. These lesions result in death when carried out with lethal force, or, if the patients live, they may leave them with serious sequelae, such as brain damage, seizure disorders, or incapacitated in a chronic vegetative state.
Brain hemorrhages can form subdural or epidural hematomas, depending on whether they occur above or under the dura mater, the membrane covering the brain. They can be equally lethal by compressing the brain and causing swelling and cerebral herniations (pressure-induced brain shifts) in turn resulting in compression of vital centers ultimately causing chronic vegetative conditions or death. Acute subdural and epidural hematomas frequently require emergency surgery. But even when successfully treated, they may leave the patients, usually younger people, disabled or incapacitated. They can also be fatal, depending on the force of the injury and on how soon the victim-patient makes it to the operating table. The mortality of acute subdural hematomas ranges from 30% to 75%.[1] Admittedly, much of the lethality at the high end of the spectrum occurs with motor vehicle accident, but it also occurs with severe beatings during assaults and the commission of crimes.
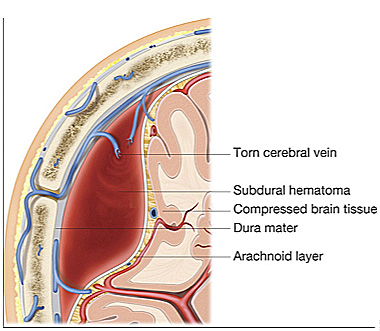
Subacute or chronic subdural hematomas, on the other hand, occur in older people, also as a result of blunt head trauma, and are very common, even after relatively minor injuries. This occurs because as we age the brain sags, the subdural space enlarges, predisposing older folks to the tearing of the bridging veins at the top of the head inside the skull. [Figure 3] Chronic subdural hematomas can occur after relatively minor injuries or even after a vigorous struggle or simply the shaking or bumping of the head during a scuffle with an assailant.
Sometimes difficult to diagnose, subacute and chronic subdural hematomas may present in older victims days or weeks after an assault. Yet these hematomas can also cause severe brain damage, incapacitation, or death. In other words, a serious or mortal injury can occur when a weaker person is attacked by an assailant who is intent on injuring or incapacitating his target, male or female, to rob them or sexually assault them.
Violence is rampant and endemic. Assault in the streets or during home invasions, whether the object is robbery or rape, frequently takes defenseless persons by surprise. The best defense is ready, armed defense. The firearm must be immediately available, usually concealed for self-defense outside, or kept in a secure place inside the home. Criminologists have determined that a firearm is the most effective weapon of defense against violent assailants.[2-5]
In dealing with these assault cases, one must also keep in mind that a person bent on attacking and victimizing another person carries the advantages of timing, selection, and purposeful intent. They are intent on hurting, robbing, or raping their victims. Thus they have the advantage of having selected the time, place, and the victims themselves.

Victims do not expect the attack and are often taken by surprise. Frequently, assailants are younger, more agile, and stronger than their victims (whom they have picked as suitable targets). Smart unarmed assailants would hesitate from physically assaulting an Arnold Schwarzenegger or a Jesse Ventura, but not a frail individual whom they believe they can successfully victimize. Even an unarmed predator can wield deadly force with his hands, feet, or other simple objects easily carried. A stolen candle stick in the hands of a determined assailant should be considered a lethal weapon and treated as conveying deadly force, especially when the assailant has entered or broken into a home and the victim, male or female, reasonably feels threatened and in mortal danger.
As I wrote many years ago, criminologists have noted:
National Victims Data suggests that “while victims resisting with knives, clubs, or bare hands are about twice as likely to be injured as those who submit, victims who resist with a gun are only half as likely to be injured as those who put up no defense.”
Similarly, regarding women and self-defense, “among those victims using handguns in self-defense, 66% of them were successful in warding off the attack and keeping their property. Among those victims using non-gun weapons, only 40% were successful.
Among those victims fleeing the scene, only 35% were successful. Among those victims invoking physical force, only 22% were successful. Among those using verbal shouting only 20% were successful…” The gun is the great equalizer for women when they are accosted in the street or when they are defending themselves and their children at home.
When severe bodily injury and blunt head trauma are a possibility, deadly force used in self-defense is warranted and morally justified.[6] And the safest and most effective defense is with the use of firearms by the intended victims, that is, by citizens who know how to use firearms and are determined beforehand to protect themselves and their families from predators. Such unpredictable violence should be considered capable of causing grave bodily harm and blunt head trauma. Neurosurgical complications of head injuries may include seizure disorders, paralysis, blindness, and mental and emotional problems that result as sequelae of brain injuries, not to mention the death of the victim.
In short, guns are the great equalizer for both men and women assaulted by criminal predators, who hold the advantage in acts of violence, and purposely inflict bodily harm in the commission of their crimes. Thus, when persons with hostile intent break and enter a home threatening bodily harm or injury, the victims are justified in using deadly force for self-defense and family protection. Business establishments that forbid the carrying of arms by persons possessing a valid concealed carry license and who wish to exercise their right while patronizing the premises should be held legally responsible when customers are harmed or killed because their right to self-defense was denied.
It’s time that the public, prosecutors, defense attorneys, juries, legislators, and the police understand that blunt trauma to the head can be potentially crippling or lethal during a scuffle with a criminal, and that the use of deadly force by the potential victim is often needed and almost always justified for self-defense and family protection.
References
1. Faria MA. Tindall GT. Evacuation of subdural hematoma. In: The Medical Management of the Surgical Patient. Lubin, Walker, and Smith (editors). Boston, MA: Butterworth Inc., 1982.
2. Kates DB, Harris PT. How to make their day. National Review 1991;43(19):30-32.
3. Kleck G. Point Blank: Guns and Violence in America. New York, NY: Aldine de Gruyter, 1991.
4. Lott JR. More Guns Less Crime: Understanding Crime and Gun Control Laws.” Chicago, IL: University of Chicago Press, 1998.
5. Wright J., Rossi P. Armed and Considered Dangerous: A Survey of Felons and Their Firearms, New York, NY: Aldine de Gruyter, 1986.
6. Saint Thomas Aquinas. Summa Theologica, II, Ch. 64, Art. 7
Written by Dr. Miguel Faria
Miguel A. Faria, Jr., M.D. is an Associate Editor in Chief and World Affairs Editor of Surgical Neurology International (SNI). He is Clinical Professor of Surgery (Neurosurgery, ret.) and Adjunct Professor of Medical History (ret.), Mercer University School of Medicine. Dr. Faria was a member of the Injury Research Grant Review Committee of the Centers for Disease Control and Prevention (CDC; 2002-05). He is the author of Vandals at the Gates of Medicine (1995); Medical Warrior: Fighting Corporate Socialized Medicine (1997); and Cuba in Revolution — Escape From a Lost Paradise (2002). His website is https://haciendapublishing.com. His most recent book is America, Guns, and Freedom (2019).
This article may be cited as: Faria MA. Potentially lethal force may require defensive deadly force. DRGO.us, February 9, 2016. Available from: https://haciendapublishing.com/potentially-lethal-force-may-require-defensive-deadly-force
First published February 6, 2016. A version of this article also appears in DRGO.
Copyright ©2020 Miguel A. Faria, Jr., M.D.