Vaccines — Kill or Cure?
As the controversial debate over mandatory vaccine policy heats up igniting passions, it is perhaps appropriate we summarize what is known about the manifest benefits of modern vaccines, not forgetting the tremendously salutary impact on health and longevity wrought about by better living conditions, hygiene and sanitation, in general, and the introduction and subsequent widespread use of antibiotics, in particular.
In Part I of this essay, we discussed the history of vaccinations, the advent of the germ theory of disease, and the ushering in of the dawn of scientific medicine.1 In Part II, we will weave into this historic tapestry the more contemporary history behind some of the many infectious illnesses of the 20th century and revisit the story as to how they were eradicated. Only then can we arrive at today’s reality over vaccine policy and reach the truth as to the best possible advice that should presently be given to individual patients.2,3
Officials at the CDC tell us vaccines are “90 percent safe and effective.” And according to UNICEF, vaccines save the lives of at least 1.5 million children every year. Yet, parents are concerned, and increasingly, dissenting physicians are asking questions and breaking away from the heretofore monolithic medical ranks. Let’s look at the big picture to avoid missing the forest for the trees.
Growing up, I thought deadly infectious diseases had been conquered long ago. Yet, in Cuba, I knew of a girl who died of diphtheria, and my father as a country doctor, diagnosed and treated a case of anthrax and another one of typhus. When I visited Haiti in 1975 as a medical student, I saw cases of tetanus and congenital syphilis. In 1982, while I was chief neurosurgical resident at Grady Memorial Hospital in Atlanta, Georgia, we had in our service, simultaneously, patients with Pott’s Disease, miliary TB with renal involvement and cerebral tuberculoma (for which we were consulted as to possible removal), and tubercular meningitis (for which we were to implant a Rickham reservoir for CNS chemotherapy). Scrofula was the only “classical” TB case missing in our clinical service!
And with the advent of AIDS and other immune deficiency and immunosuppressed states, we have seen in the 1990s a resurgence of tuberculosis and other opportunistic, infectious diseases, e.g., toxoplasmosis, cytomegalovirus (CMV), etc. In my own practice, I treated patients with chronic fungal meningitis and bacterial subdural empyemas requiring surgical evacuation. So, infectious diseases are still with us, and so taking preventive public health measures is prudent in many circumstances when the public is at risk. With this in mind, let’s look at some of these diseases that are specifically salient to our discussion, and try to separate the wheat from the chaff in the debate.
Poliomyelitis
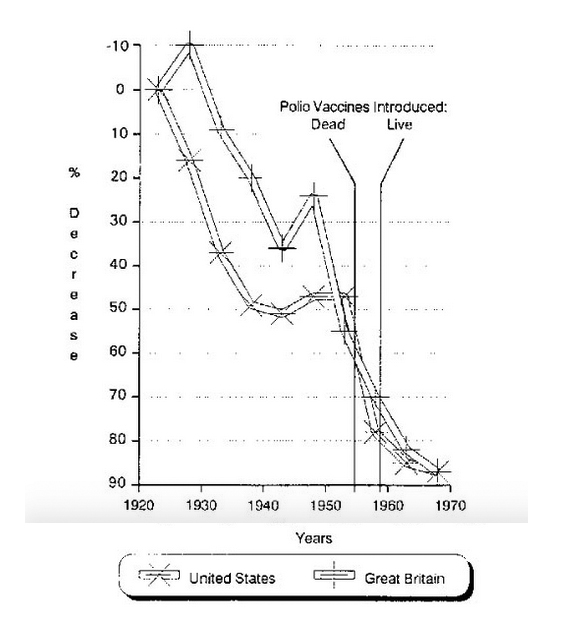
In the 1950s, there were 20,000 cases of polio annually causing more than 1,000 deaths4; many more thousand victims were left in iron lungs. This was caused because of the predilection of the polio virus for the anterior horn cells of the spinal cord and consequent paralysis of the respiratory muscles. But, what is less known, and this is quite disconcerting to me, is that between 1923-1953, before the Salk (dead virus) vaccine was discovered in 1955, the polio death rate in the U.S. and England declined on its own by 47 percent and 55 percent, respectively.5 This is not reported or discussed by the public health establishment but, it seems, only by independent researchers [Figure 1]; neither is the fact that European countries, which didn’t systematically immunize their citizens, also experienced a precipitous decline in their polio morbidity and mortality statistics.
And yet, between 1951-1954, before immunization, there were still more than 16,000 cases of polio and nearly 1,900 deaths. It was not until 1991 that polio was virtually eradicated from the U.S. and other nations of the Western Hemisphere. There is no question that in this case better hygiene and sanitation and better living conditions were bringing down the number of cases of polio, but the vaccine itself, finally, was probably responsible for dispatching the final blows to the disease.
Today the disease has been completely eradicated, except for the fact that with the advent of the Sabin (live virus) vaccine in 1959, there had been iatrogenic cases of polio (up to 8 cases per year) that had developed due to activation and infection by the live oral polio virus in the vaccine. Due to this fact, in June 1999, the CDC and the American Academy of Pediatrics (AAP) began advising doctors to use the Salk (dead virus) injected vaccine rather than the oral vaccine containing the live virus.6
Diphtheria, Tetanus, and Pertussis
Diphtheria is caused by Corynebacterium diphtheriae. The disease begins with a sore throat, fever, and lymphadenopathy that progresses swiftly to respiratory distress by the formation of an occluding membrane in the nasopharynx and generalized muscle paralysis that may result in respiratory arrest. The average annual number of diphtheria cases in the U.S. between 1920-1922, the three years before vaccine development, was 175,885.
Between 1900-1930 before the diphtheria vaccine, greater than a 90 percent decline was noted in this disease by practicing physicians due to better diet, living conditions, and sanitation,5 and yet there is no question the diphtheria toxoid played a significant role in conquering the last 10 percent of fatal cases of this disease. In 1998, there was only one case in the U.S.
Similar cases can be made for tetanus and pertussis, the two other diseases targeted by the DPT (Diphtheria, Pertussis, Tetanus) immunizing agent mixture of precipitated toxoids.
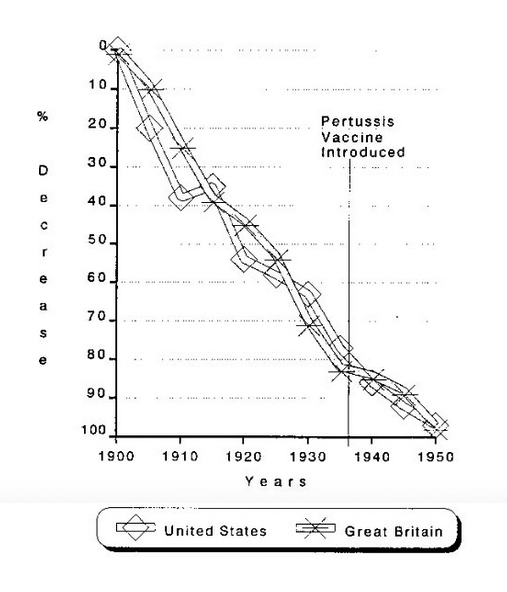
The average annual number of pertussis (whooping cough) cases between 1922-1925 (the 4 years before vaccine development) was 147,271. By 1998, this figure had fallen so that there were 6,279 cases in the U.S.
And yet, the incidence and severity of pertussis had been declining before the pertussis vaccine was introduced. From 1900-1935, in the United States and England, before the vaccine program for whopping cough had been implemented (in the 1940s), the death rate from this disease had already declined by 79 percent and 82 percent, respectively [Figure 2].5
Unfortunately, despite the great advances in Western nations, as many as 9,000 people, particularly children, still die annually from whopping cough mostly in Third World countries.
The same may be said for lockjaw (tetanus). The estimated average annual number of cases between 1922-1926 was 1,314. By 1998, U.S. tetanus cases had dropped dramatically to 34. Yet, this disease is still with us in undeveloped nations because of poor living conditions.
Mumps, Rubella and Measles
According to the public health figures, the number of mumps cases in 1968 (the year reporting began and the first year after vaccine licensure) was 152,209. We also learn that by 1998 there were 606 cases in the U.S.4 Immunity to mumps is acquired naturally or through the mumps, measles, and rubella (MMR) vaccine.
The average annual number of rubella (German measles) cases between 1966-1968, the 3 years before vaccine licensure, was 47,745, and there were 345 cases in the U.S. in 1998. The estimated average annual number of cases of congenital rubella syndrome between 1966-1968, the 3 years before vaccine licensure, was 823. By 1998, there were only 5 cases in the U.S.
During the 1964-1965 season, before immunization to German measles was available, 20,000 infants suffered from an outbreak of congenital rubella with deafness, blindness, and mental retardation. They contracted their disease as babies from infected mothers in uterus. Otherwise, rubella had not been a particularly difficult illness (i.e., when acquired naturally as a childhood disease). In fact, it’s self-limited and frequently so mild it can escape detection. Congenital rubella in newborns is a different and more devastating disease than the childhood illness. Prevention is geared toward preventing expectant mothers from getting rubella and avoiding its transmission in uteri to their babies. MMR has been effective in reducing the incidence of these diseases and controlling outbreaks, although routine public health measures e.g., better hygiene and sanitation cannot be ignored.
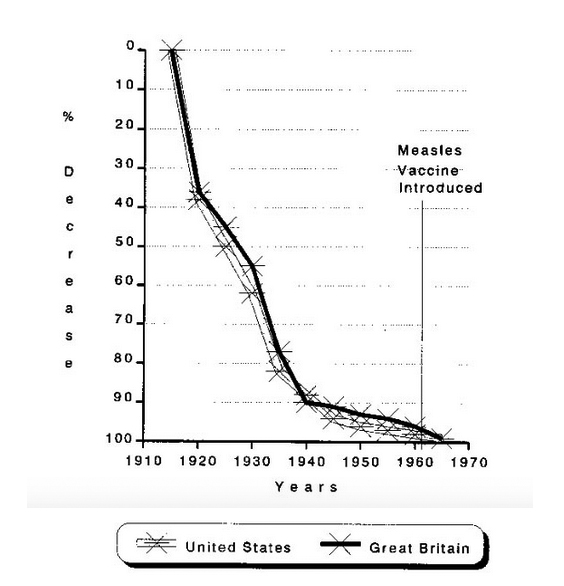
From 1958-1962, before the measles (attenuated live virus) vaccine, an excess of 500,000 Americans contracted the virus annually and suffered the illness, according to government figures. Although for most children contraction of this usually self-limited illness was a rite of passage, for some, 1 per 1,000, it led to complications, the most dramatic being measles encephalitis. With the advent of the measles, mumps, rubella vaccine (MMR), the government reported there were only 89 cases in 1998. Not everyone agrees with this assessment, and again independent researchers counter that a significant decline in measles took place before vaccination was introduced in the United States and England. And, in fact, before the inception of the measles vaccine (1963), from 1915-1958, a 95 percent decline took place in measles death rate [Figure 3]. That is, the measles death rate dropped from approximately 13.3 deaths per 100,000 population in 1900 to 0.03 deaths per 100,000 in 1955. Moreover, post-vaccination death rates for measles in the mid-1970s are similar to those of the pre-vaccination years in the early 1960s.5
Public health and the press have nothing but praise for vaccination programs, even mandatory immunization. For example, a recent (but typical) newspaper article reports: “Many Americans have either forgotten or never lived through the periods when children used to die from outbreaks of diseases such as measles or polio.”7 In this instance, the reporter quotes Dr. Walter Orenstein, director of the CDC’s National Immunization Program, who noted that in a regional epidemic of measles in Los Angeles peaking as late as 1990, 4,549 cases of measles were reported with 12 deaths. The point being that the disease is still there and dangerous. Yet, Barbara Fisher, president of the Vienna, Virginia-based National Vaccine Information Center (NVIC), countered that during this measles outbreak (1989-1990), “a whole group of young mothers who had been vaccinated against measles, and therefore only had temporary, artificial immunity were not able to give their babies the protection unvaccinated mothers had given them. We saw a lot of measles in very young babies where they did not naturally occur before.”8 In other words, active immunization did not provide mothers with the long lasting immunity that is provided by acquiring the disease naturally.
In some of these infants, she speculated, the mother wasn’t able to pass her immunity to them as babies because they had not contracted and overcome the natural measles virus during their childhood and therefore couldn’t pass this immunity on to their babies, who otherwise would have been protected for 12-15 months after birth.
Smallpox
The conquest of smallpox is one of the great triumphs of public health and immunization, as I described in Part I of this article.1 The disease has now been completely eradicated from the world.
In 1900, 21,064 cases of smallpox were reported in the U.S. of which 894 persons died. According to the CDC, the average annual number of smallpox cases between 1900-1904 was 48,164.4 There have been no reported cases of smallpox in the U.S. since 1950, and no cases worldwide since 1977. Routine vaccination for smallpox ended in 1971. Dr. Jane Orient tells me that the U.S. government has somewhere in storage over a million doses of the vaccine, but whether they are still effective is open to question.
Chickenpox (Varicella)
Chickenpox is a childhood illness which confers lifelong immunity to most children it afflicts without serious complications. The vaccine’s “duration of protection is unknown at present, and the need for booster doses has not yet been clearly defined. Moreover, vaccination is considered unnecessary by many authorities because 95 percent of American children get it by age 9. And the illness is not particularly difficult for children. In fact, the American Academy of Pediatrics (AAP) as late as 1996 instructed in its immunization brochure that “most children who are otherwise healthy and get chickenpox won’t have any complications from the disease.” It is speculated the chickenpox vaccination has been implemented to reduce the number of work hours parents lose by staying home tending to their sick children. The chickenpox vaccination was added to the children’s immunization regimen in 1995.
Rotavirus (Diarrhea) Vaccine
About 1 million infants were immunized with RotaShield between its approval in September 1998 and its suspension in July 1999 because of its etiological link to severe intussusception in babies. Fifty-three of these infants required surgery, two died, and another 47 required urgent medical attention for their bowel obstruction caused by the vaccine-induced intussusception. The Rotavirus vaccine was discussed in a recent issue of the Medical Sentinel.9
Hepatitis B
The risk of infants contracting hepatitis B is close to non-existent. Yet, serious adverse effects from the vaccine, including 48 deaths, are being reported three times as frequently as cases of hepatitis B in children under the age of 14. This immediately begs for the question of why? There is no question the vaccine is appropriate for high risk populations such as prostitutes and IV-drug abusers; police and medical emergency personnel, who may come in contact with infected blood; as well as surgeons, nurses and health care workers, because these are high risk occupations, but why newborn infants with extremely immature immune systems and who, being so young, are not exposed to the risks of contracting this disease?
Recently, the AAP and the U.S. Public Health Service have come to their senses and changed their policy regarding hepatitis B vaccination: Mothers are to be tested during pregnancy, and if they are negative for hepatitis B, then the child’s vaccine may be delayed until age 6 months. Nevertheless, Parents Requesting Open Vaccine Education (PROVE), an Austin, Texas-based grassroots organization founded in 1997, have objected to the fact that “parents in Texas and many other states, based on their own assessment of disease versus vaccine risks, don’t have a legal right to personally exempt their children from the hepatitis B vaccine which is now required for most school children entering kindergarten.”8 Furthermore, this group remains concerned because 10,000 to 12,000 reports of vaccine reactions are added each year to a federally run vaccine database, and of this, roughly 20 percent are classified as serious.10
Federal guidelines issued in 1991 and still in place recommend 3 doses of the hepatitis B vaccine for health professionals, who come into contact with blood, and individuals at risk, e.g., drug abusers, people with multiple sex partners, as well as every child born after 1990.11
In fact, for the year 1996, the CDC reported only 54 cases of the disease occurring in infants under age 1, out of 3.9 million births that year,10 and at a U.S. congressional committee on Government Reform (May 18, 1999) looking into the problems of hepatitis B vaccines, a CDC official disclosed there were only 279 cases of hepatitis B under age 14 that year. The total annual incidence of hepatitis B is estimated at between 150,000 to 300,000 by the same government official. Although the published figures in the MMWR for 1997 is 10,000 hepatitis B cases, the CDC states that the “vast majority of cases go unreported because the hosts are asymptomatic or mistake the reaction for the flu.”11
Hepatitis A is a disease transmitted by the fecal/oral contamination route, primarily via unwashed hands after toilet use or the handling of contaminated food or water. Recently, infants living in Texas and Oklahoma, bordering with Mexico are required to be immunized against this disease, although the duration of protection has not been established, and it’s unknown whether immunity will even last until adulthood.
Then there is insidious hepatitis C (HCV, formerly known as hepatitis non-A, non-B). A recent article in Science reports that worldwide hepatitis C afflicts some 170 million people with an infection rate 4 times as high as for HIV: “In the U.S., the annual death rate for HCV-caused cirrhosis or liver cancer may overtake that from AIDS within the next few years.”12 In the U.S., HCV causes 8,000 to 10,000 deaths annually and accounts for the largest number of liver transplantations. Of the 75-85 percent of patients that continue to have chronic hepatitis C after a bout with this enigmatic disease, 20 percent eventually develop cirrhosis and 1 to 5 percent liver cancer. The problem with HCV is that it is genetically different from hepatitis B and there are more than 100 strains, making vaccination research and development efforts difficult, if not futile at this time. Hepatitis C poses a threat to the world, a fact underscored by its transmission via blood transfusions before a screening blood test was developed in 1990. While sexual transmission may or may not occur, the most common modes of contracting this disease are contaminated needles and perinatal transmission which occurs in about 6 percent of babies born to infected mothers.12
Typhoid Fever, Typhus and Cholera
Typhoid fever and typhus are completely different diseases. And yet, while bacteria cause typhoid fever and rickettsias typhus, both afflictions have been associated with poor hygiene and sanitation and have been confused clinically in the past. During the Spanish American War in 1898, more men were lost to typhoid fever than were killed in battle. Much of the same can be said about typhus in World War I. Cleanliness, improved hygiene and sanitation and better living conditions conquered both of these diseases; although DDT, the much maligned pesticide, had a significant impact in controlling typhus (body lice), just as it did malaria (Anopheles mosquitoes) by eliminating the insect vectors. Clean potable water along with proper disposal of sewage played major roles in controlling typhoid fever and cholera.
Although much has been said about overcrowding in urban, industrial areas, the advent of the Industrial Revolution was a formidable event working against most infectious diseases. It brought an improved standard of living, better nutrition, cheap soap, and inexpensive cotton clothing, clothing which could now be washed and rendered free of lice — all of which contributed significantly to the eradication of typhus.13 The use of effective antibiotics such as chloramphenical and tetracycline (along with re-hydration in cases of cholera) were pivotal factors for those already ill with these diseases. Vaccinations for these agents in targeted populations has been helpful, but did not play the same critical role as these aforementioned measures.
Tuberculosis
Between 1930 and 1987, such diseases as syphilis, pneumonia, typhoid fever and typhus and the old consumptive killer, tuberculosis, were controlled, not only because of better hygiene and sanitation but also because of the newly developed antibiotics. Vaccines played an insignificant role, if any at all with these diseases.
Tuberculosis, the White Death, dropped from the top of the list of human killers to #21 in the morbidity and mortality statistics during the middle of the century. As a result, life expectancy climbed from 59.7 years in 1930 to 74.9 years by 1987.13
Before the advent of scientific medicine, tuberculosis was a devastating and dreaded disease. The dreaded illness had been, in fact, christened the White Death because the skin of those afflicted turned alabaster white, thin and translucent, making small veins visible. The White Death took both the poor and rich, the destitute and the affluent, the masses and the intellectuals. The Who’s Who of 19th century European literature succumbed to this disease including, Anthony Trollope; Emily, Anne, and Charlotte Brontë; Henry David Thoreau, Frédéric Chopin, John Keats, Franz Kafka, and many others. The year Existentialist philosopher Franz Kafka died in 1924 there were over 200,000 Americans who also died from tuberculosis. The conquest of tuberculosis at that time was not due to vaccination with BCG (Bacille Calmette-Guérin) a live, attenuated mycobacterium strain, which was developed later in the 20th century. This vaccine has not been proven to be uniformly effective. The conquest of TB was due to the advances made in understanding the pathogenesis of tuberculosis and its milieu, better education, isolation, use of x-ray, the old standbys — better hygiene and sanitation — and, of course, the use of effective antibiotics e.g., streptomycin (1952), isoniazid (1953), and rifampin (1969).
In the 1990s, there was a resurgence of TB among the immunocompromised AIDS patients. Moreover, there was a multiple drug resistant (MDR) strain of tuberculosis reported in the U.S. in 1992, and although the situation seems to have stabilized, MDR TB continues to be reported in infected immigrants entering the U.S.
In 1998, TB incidence was 6.8 per 100,000 people, and immigrants, barely 10 percent of the American population, accounted for 42 percent of the 18,361 reported cases of tuberculosis in the U.S.
Multiple drug resistant TB continues to be reported with increased frequency in Europe, Asia (particularly communist China), and Africa.14
The Surgeon General, David Satcher, M.D., tells us, “We must therefore approach it as a global, public health problem, partnering with multi-national organizations, the pharmaceutical industry, and other nations to seek solutions.”15

AIDS
Despite the publicity given this affliction and the politicization of this disease, the total number of victims of Acquired Immune Deficiency Syndrome (AIDS) has topped 400,000 in the U.S., a high number, but it has taken nearly two decades to reach this number. By comparison, tuberculosis claimed 200,000 lives in a single year in a country with a much smaller population. An estimated 10.7 million people are infected with both HIV and tuberculosis.15
As of March 1999, there have been 700,000 cases of AIDS reported since January 1981, the year the epidemic began. Last year (1998) there were about 48,000 new cases reported and approximately 20,000 deaths. While medical researchers have arduously sought a vaccine, no major breakthrough has taken place yet. If the U.S. develops vaccines against HIV, they may be recommended to the entire population since presumably “we are all at risk of AIDS.”
In Africa, AIDS (with HIV type II, a different virus common in heterosexuals), a true pandemic, has spread like a wild fire because of the virulence of this virus as well as cultural lifestyle differences. In the Central African Republic, Zimbabwe and other African nations, the infection rate may be as high as 30 percent according to the World Health Organization (WHO); in another report, testing of military units in Zimbabwe revealed a 90 percent infection rate.16
Additional Vaccines Coming Down the Pipe
There is research being conducted for more than 200 vaccines, many of which may be considered for mandatory administration.17 These include herpes, chlamydia, and even cocaine addiction! Regarding this latter malady, Dr. Kristine Severyn at the 56th annual AAPS meeting in Coeur D’Alene, Idaho in 1999, reported that conceivably this vaccine would be given to all children to avoid embarrassing those who have high risk parents and thus may potentially suffer diminution of their self-esteem.
Between 1963 to 1998, there have been six new vaccines added to the mandatory vaccine regimen already in place in the U.S. This vaccine schedule now includes: 1) DPT (Diphtheria, Pertussis, Tetanus) total of 5 doses; 2) 5 doses of live oral polio (Sabin) should already have been replaced by the Salk (dead virus) vaccine shots by January 1, 2000; 3) 2 doses of live measles, mumps, and rubella (MMR); 4) 4 doses of Hemophilus influenzae type B (Hib). This vaccine was approved in 1990 to prevent Hemophilus meningitis in children; 5) 3 doses of hepatitis B vaccine; 6) Between September 1998-July 15, 1999, when it was discontinued, children also received three oral Rotavirus diarrhea vaccine; 7) Chickenpox was added to the regimen in 1995 and consists of a single dose.
By different counts it is estimated that between 21 to 33 doses of vaccinations are given to children and infants before the first grade. Could these vaccines adversely affect the developing immune systems of infants and young children? Many authorities believe that this is so, although there is no absolute scientific proof as of yet that this is the case.
During the period 1963-1998, immunization rates for American children under age 3 rose from between 60 and 80 percent in 1967 for MMR, polio, and DPT to between 80 to 95 percent for these vaccines, as well as the Hib and hepatitis B vaccines, according to the Morbidity and Mortality weekly report of the CDC.18 And until July 1999, infants were inoculated with hepatitis B vaccine shortly after birth, but as we mentioned earlier, the AAP and the CDC have recommended that this vaccine now be held until age 6 months.
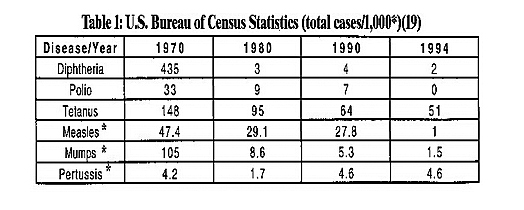
Before children can enter kindergarten, they are required by law in all 50 states to be immunized with a complicated regimen of a variety of viral and bacteria immunization agents against at least nine contagious illnesses. The following chart shows figures for the number of cases per 1,000 of various contagious illnesses reported between 1970-1994. It shows a progressive decline in the incidence of most of these illnesses: diphtheria, polio, tetanus, measles, mumps and pertussis, as a result of preventive public health measures including vaccines [Table 1].19
Nevertheless, concerns remain. It was the swine flu vaccination tragedy in 1976 that precipitated a rash of cases of Gillain-Barré syndrome, and elicited the first signs of concerns from the public. Since then, the CDC’s own reported figures show 10,000 to 12,000 vaccine reactions occurring annually (of which 20 percent are serious). And even these figures are questioned. Barbara Fisher, president of the NVIC, asserts “even the FDA has acknowledged that only 10 percent of all adverse reactions are reported.”8
And there is more. There are the disturbing reports by advocacy groups as well as independent researchers that raise the possibility of casual links between MMR and DPT (particularly the pertussis portion) and asthma20 and autism21; diabetes and the meningitis Hib vaccine22,23; and between the hepatitis B vaccine and multiple sclerosis, chronic fatigue syndrome, rheumatoid arthritis, and other autoimmune disorders.24-28 Although the CDC reports that all these claims have been investigated and remain uncorroborated, the skepticism and concern remains.

The Anthrax Controversy and the Threat of Bioterrorism
I would be remiss if I didn’t list and mention anthrax. In Part I of this article, we discussed anthrax in relation to the historic contribution of Dr. Louis Pasteur. Today, anthrax is at the vortex of the vaccine controversy because many military personnel are refusing to be vaccinated against this disease, despite expressed orders to do so. Anthrax has not only been considered suitable for biological warfare, but an ideal agent for bioterrorism, because the organism is one of the deadliest bacteria known to man and its spores are extremely resistant, almost indestructible.
Although the usual strain of anthrax is sensitive to ordinary antibiotics, such as doxycycline or ciprofloxacin, the new strains are resistant, making U.S. troops vulnerable to enemy attack, particularly in the volatile and dangerous Middle East, where dictators such as Saddam Hussein of Iraq are believed to possess stockpiles of the virulent organism. Moreover, uncorroborated rumors have been circulated that genetically altered strains have been created in the laboratory for germ warfare. Needless to say, our troops could be at risk when they are sent to troubled spots around the world by the UN as “peacekeepers,” including the Middle East. Yet, military personnel have been court-martialed rather than receive the anthrax vaccine because of safety concerns, including the belief that the vaccine is related to the nebulous disease complex referred to as Gulf War Syndrome.29,30 Although textbooks of military medicine state the vaccine is “safe and effective,”31 this assertion is refuted by other authoritative texts. For example, one text states the current vaccines are impure and chemically complex, elicit only slow onset protective immunity, provide incomplete protection, and cause significant adverse reactions.”32
Conflicts of Interest
One of the most troubling aspects of the issue of vaccine policy is the cozy public-private partnership developing between supposedly disparate interests, militating for what an article in The Village Voice refers to as the rise of the Vaccine Nation and the concomitantly arising conflict of interest in this “partnership.” The relationship extends all the way to organized medicine where AMA past president Nancy Dickey, M.D. has called for a new public-private partnership between public health and (organized) medicine: “As our health system has developed, there have been few incentives for collaboration and interaction between medicine and public health. So what has happened is that public health now zeroes in on certain populations and certain aspects of health care while the doctor continues to treat illness on a case-by-case basis. But the rising costs of health care and the dominance of managed care in medicine and public health are creating a new reality for all of us…Medicine and public health must re-evaluate our relationship — because in today’s increasingly complex, dollar-driven world — we can no longer accomplish our missions alone.”33
But let us return to the serious conflict of interest implications raised in The Village Voice article which states:
Clearly, the rise of the Vaccine Nation represents a boon for public health, but it also offers untold opportunities for profit. In 1997, vaccine sales brought in about $1 billion for Merck, the leading vaccine manufacturer, and the industry now has about 42 new vaccines in the pipeline. Last year, the twin goals of public health and profiteering converged in the form of the Vaccine Initiative, a PR campaign launched by several medical societies to promote universal immunization. Last week, the group adopted a new name, the National Immunization Information Network (NIIN), after attracting new partners and replacing its startup grants from vaccine manufacturers with funding from the Robert Wood Johnson Foundation, the philanthropic arm of Johnson and Johnson.34
The article went on to report how The New Yorker magazine which had joined the Robert Wood Johnson immunization bandwagon along with The Wall Street Journal, The New York Times, and The Washington Post, contained its pro-vaccine pieces adjacent to health-related ad sections of the pharmaceutical industry’s leading trade association (PhRMA), whose marketing tag line reads, “America’s pharmaceutical companies: Leading the way in the search for cures.”34
Before 1960, there were only a few vaccines that were administered for rampant diseases that were known to have posed a clear and present danger, an immediate and imminent epidemiologic threat. Today, it seems that the public health establishment is obsessed with developing vaccines against every conceivable microorganism, and these government programs are bent to include everyone, every child, every infant in the immunization loop. And yet, at this time, the medical evidence should tilt the balance of the debate towards the government allowing parents and individuals to be armed with reliable vaccine information. So empowered, as individuals and masters of their own destiny, citizens and parents should be allowed to make their own decisions or those of their children with their private physicians. As an AAPS physician explained back in 1960 regarding the issue of immunization: “I am certain of one thing, that the most fundamental element in our American system of medical care is mutual responsibility of a personal physician and that individual patient to his physician. This mutual interest is not served by a scramble for “free” production line care, but by a personal visit by a doctor’s personal patient to his personal doctor.”35
Thus in concluding, perhaps, it is worth repeating: . . . the pages of medical history are replete with indisputable evidence that physicians, upholding the Oath and individual-based ethics of Hippocrates, actually benefit not only their individual patients but also society, secondarily. In other words, physicians working in the enlightened best interest of their patients actually result in tangible benefits to humanity as a whole. On the other hand, the historic record also reveals, in this very century, when that is not the case and physicians become agents of the state, rather than advocates of their patients, events go awry. Physicians become preoccupied with preventive health measures and the so-called proper allocation of scarce resources, rather than the health of their individual patients. The result is that medicine becomes subordinated to, and physicians act as agents of, the state, a situation that is as perverse as it is disastrous. It’s time physicians choose: In vaccination, as in everyday practice, is it the dictate of your conscience to abide by the individual-based Oath and ethics of Hippocrates or to comply with the collectivist morality of population-based medicine?1
References
1. Faria MA, Jr. Vaccines (Part I): Jenner, Pasteur, and the dawn of scientific medicine. Medical Sentinel 2000;5(2):44-48. Available from: https://haciendapublishing.com/vaccines-part-i-jenner-pasteur-and-the-dawn-of-scientific-medicine/
2. Schlafly R. Official vaccine policy flawed. Medical Sentinel 1999;4(3):106-108.
3. Orient JM. Mandating vaccines — government practicing medicine without a license? Medical Sentinel 1999;4(5):166-168.
4. Morbidity Mortality Weekly Report, April 2, 1999. http://www.cdc.gov/mmwr/
5. Miller NZ. Vaccines – Are They Really Safe and Effective? Santa Fe, NM, New Atlantean Press, 1992, pp.17-35. http://www.thinktwice.com. See also Mendelsohn R. How To Raise A Healthy ChildIn Spite of Your Doctor. Chicago, IL., Contemporary Books, 1984, pp. 216, 219, 228; Alderson M. International Mortality Statistics. Washington, DC, Facts on File, 1981, pp. 82-83, 164-165, 177-178 ; Cherry J. The new epidemiology of measles and rubella. Hospital Practice, July 1980, p.49; and Moskowitz R. Immunizations: the other side. Mothering, Spring 1984, p. 36.
6. Manning A. Parents fear growing number of vaccines. USA Today, August 3, 1999.
7. Orenstein W. quoted by Allen J. in Shots in the dark — can childhood vaccinations cause devastating illnesses? Los Angeles Times, October 18, 1999.
8. Fisher B. quoted by Cameron F. in Infant vaccinations: A biological assault? Health and Nutrition Breakthroughs, January 1999. http://www.hnbreakthroughs.com/jan99/vaccine.cfm.
9. Rotavirus vaccine. Medical Sentinel 2000;5(1):4.
10. Morbidity Mortality Weekly Report 1996. http://www.cdc.gov/mmwr/
11. Howd A. Ounce of prevention, pound of misery? Insight, March 12, 1999.
12. Science 1999;25:26-30, cited and summarized in Civil Defense Perspectives. Physicians for Civil Defense 1999;15(5):1-2.
13. Faria MA, Jr. Medical Warrior: Fighting Corporate Socialized Medicine. Macon, Georgia, Hacienda Publishing, Inc., pp. 127-131.
14. D’Agostino JA. Will tuberculosis find an open border? Human Events, Jan. 14, 2000.
15. Satcher D. Tuberculsos – battling an ancient scourge. JAMA 1999;282(21).
16. Monteith S. AIDS: the untold story. Medical Sentinel 1997;2(3):97-99.
17. Phyllis Schlafly Report. Part I – Whatever happened to informed medical choice? And Part II – Vaccines, a miracle of modern medicine? February 1999.
18. Morbidity Mortality Weekly Report, April 2, 1999. http://www.cdc.gov/
19. U.S. Bureau of Census Statistics and Statistical Abstracts of the U.S., 116th edition, Washington, DC, 1996.
20. Odent MR, Culpin EE, Kimel T. Pertussis vaccinations and asthma: Is there a link? JAMA 1994;272:588-592.
21. Wakefield AJ, et al. Ileal-lymphoid nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. The Lancet 1998;351:637-641.
22. Karvonen M, Cepaitis Z, and Tuomilehto J. Association between type 1 diabetes and hemophilis influenza type B vaccination: birth cohort study. BMJ 1999;318:1169-1172.
23. Tuomilehto J, et al. Increase in incidence of insulin dependent diabetes mellitus among children in Finland. Int J Epidemiol 1995:24:984-992.
24. Coulter H. The assault on the American child: vaccination, sociopathy, and criminality. Berkeley, California, North Atlantic Books, 1990.
25. Silverstein A. Pure Politics and Impure Science. Baltimore, Maryland, Johns Hopkins University Press, 1981.
26. Stratton K, et al. Adverse events associated with childhood vaccines: evidence bearing on causality. Washington, DC, National Academy Press, 1994.
27. Dunbar B. quoted in Ounce of prevention, pound of misery, op. cit.
28. Waisbren BA, Dunbar B. Hepatitis B vaccine: Helping or Hurting. Statements to the Subcommittee on Criminal Justice, Drug Policy, and Human Resources of the U.S. Congressional Committee on Government Reform, May 18,1999.
29. Biological weapons and vaccines. Doctors for Disaster Preparedness (DDP) Newsletter 1999;16(2):1-2.
30. Nature 1997;390:3-4 cited in DDP Newsletter, op. cit.
31. Sidell FR, Takafuji ET, Franz DR. Textbook of Military Medicine. Medical Aspects of Chemical and Biological Warfare. Part I: Warfare, Weaponry, and the Casualty. The Office of the Surgeon General, United States Army, TMM Publications, Washington, DC, 1997.
32. Harrison’s Principles of Internal Medicine cited in DDP Newsletter, op.cit.
33. Dickey N. We cannot accomplish one mission alone. AMNews, July 5, 1999.
34. Cotts C. The New Yorker joins the campaign for a disease free America — Rise of the vaccine nation. The Village Voice, October 13-14, 1999. http://www.villagevoice.com/issues/9941/cotts.shtml.
35. Elsten AW. Mass immunization — a doctor explains his views. AAPS pamphlet No. 1065, February 1999. http://www.aapsonline.org.
Dr. Faria is a consultant neurosurgeon and author of Vandals at the Gates of Medicine (1995) and Medical Warrior: Fighting Corporate Socialized Medicine (Macon, Georgia, Hacienda Publishing, Inc, 1997). He is also Editor-in-Chief of the Medical Sentinel.
This article was originally published in the March/April 2000 issue of the Medical Sentinel.
This article may be cited as: Faria MA. Vaccines (Part II): Hygiene, Sanitation, Immunization, and Pestilential Diseases. Medical Sentinel March/April 2000;5(2):55-61. Available from: https://haciendapublishing.com/vaccines-part-ii-hygiene-sanitation-immunization-and-pestilential-diseases.
Copyright ©2000-2021 Miguel A. Faria, Jr., M.D.